Sleep apnea and its complications are rated by the VA up to 100%, depending on the severity of the condition, but many veterans struggle to meet the VA requirements for obtaining compensation. Hill & Ponton explains service connection, how the VA rates sleep apnea, what can affect the disability rating percentage, and how to claim and increase VA benefits.
Sleep Apnea in Veterans
Sleep apnea, a condition where breathing repeatedly stops and starts during sleep, leading to various health issues, is a significant concern for many veterans, with over a half a million veterans service-connected for the condition. There are three types of sleep apnea affecting veterans:
- Obstructive Sleep Apnea (OSA): Caused by physical blockage of the airway during sleep. This is the most common type.
- Central Sleep Apnea (CSA): Caused by the brain failing to signal breathing muscles.
- Complex/Mixed Sleep Apnea: A combination of OSA and CSA.
Obstructive Sleep Apnea (OSA) occurs when the soft tissue in the throat collapses and blocks the airway during sleep. A 2024 study published in Sleep Health found that 21% of veterans have obstructive sleep apnea compared to just 9% of nonveterans. Deployment, TBI and PTSD increase the risk further.
The highest rates of obstructive sleep apnea were found in the Army (12.15%), followed by the Air Force (9.96%), and the Navy (9.06%). A study from the Journal of Clinical Sleep Medicine on obstructive sleep apnea among survivors of combat-related traumatic injury showed that rates of OSA diagnoses have surged since the Iraq and Afghanistan wars, driven by physical trauma, PTSD, and environmental exposures.
Central Sleep Apnea (CSA) is less common and results from the brain failing to send proper signals to the muscles that control breathing. Central sleep apnea is often linked to neurological conditions, opioid use, and traumatic brain injury – a frequent condition among veterans.
Both types are rated by the VA under diagnostic code 6847, but CSA may be more difficult to diagnose and service connect unless clearly linked to a service-related cause like TBI or PTSD. In such cases, a secondary service connection is often the most effective strategy, especially when a veteran is already rated for a neurological or mental health condition.
What Are the VA Disability Ratings for Sleep Apnea?
The Department of Veterans Affairs rates sleep apnea at 0%, 30%, 50% or 100% under Diagnostic Code 6847 of the Schedule for Rating Disabilities. Each rating is based on the severity of symptoms and treatments required.
- 0% Rating: Asymptomatic but with documented sleep disorder breathing. This is a noncompensable rating but can help get VA healthcare or service connect secondary conditions.
- 30% Rating: Persistent daytime hypersomnolence. Excessive sleepiness during the day must be medically documented and supported by lay testimony.
- 50% Rating: Requires the use of breathing assistance device such as continuous airway pressure (CPAP) machine. This is a common rating among veterans.
- 100% Rating: Applies only if the veteran experiences chronic respiratory failure with carbon dioxide retention, cor pulmonale (right-sided heart failure), or requires a tracheostomy.
The most common rating for sleep apnea in veterans is 30%, or 50% if a CPAP is required. But you can increase your rating by appealing the VA decision or by filing for related conditions that contribute to sleep apnea or make it worse.
CPAP VA Rating Proposed Changes
Under recent proposed changes to the VA rating criteria, simply using a CPAP machine will no longer automatically qualify a veteran for a 50% disability rating. Instead, the evaluation will focus on the effectiveness of the prescribed treatment, the veteran’s ability to tolerate or consistently use the treatment (such as a CPAP device), and the degree of functional impairment, including serious complications like damage to the heart or lungs.
If the new rating criteria are adopted, veterans whose sleep apnea is fully managed by a CPAP or similar breathing-assistance device will need to show ongoing symptoms despite treatment, inability to tolerate CPAP and documented functional impairment to obtain a 50% rating, instead of just the use of a prescribed device.
As of February 2026, the VA has not yet implemented these changes, but veterans should not assume that using a CPAP machine guarantees a 50% rating in future claims. Ensure that your medical records document:
- Ongoing symptoms (e.g., fatigue, cognitive impairment)
- Treatment compliance
- Functional limitations (impact on daily activities)
Important: The rating updates will not impact veterans currently receiving compensation or whose sleep apnea claims are filed before the changes are approved. If you are seeking to appeal your current decision to secure a 50% or higher rating, we may be able to help (at no upfront cost). Get a free case evaluation here.
Maximize Your Benefits
Unhappy with your VA decision? We’re here to help. Contact us for a free review of your case.
Connecting Sleep Apnea to Military Service
To obtain VA disability for sleep apnea, you will need three elements:
- A current medical diagnosis of sleep apnea (usually confirmed with a sleep study)
- Evidence of an in-service event, illness, or symptom (such as snoring, fatigue, or breathing issues)
- A nexus (medical opinion) connecting your sleep apnea to your military service
Is Sleep Apnea a Presumptive Condition?
A presumptive condition is a health issue that the VA automatically considers service connected if you served in a specific time or location. The PACT Act, passed in 2022, expanded the list of these conditions, especially for veterans exposed to burn pits and other toxic hazards. But sleep apnea is not yet on the list, even though it has been linked to burn pits and Agent Orange.
Because sleep apnea is not a presumptive condition, all veterans must provide evidence that their disability is connected to their service. This can happen through:
- Direct service connection: The condition began during or was caused by active duty. It requires documentation such as service treatment records or lay statements.
- Secondary service connection: Sleep apnea was caused or aggravated by another service-connected disability (e.g., PTSD, TBI, GERD).
Direct Service Connection
Proving that your sleep apnea began during active service is difficult, since sleep studies are rarely done during service. Evidence for a direct service connection can include:
- Service treatment records mentioning sleep complaints
- Lay statements (from bunkmates or spouses) noting snoring, choking, or gasping for air during sleep
- Post-service diagnosis with medical opinion linking symptoms back to service
A common problem veterans face is when they didn’t report sleep apnea symptoms while in service, or the record calls it “sleep trouble” without identifying apnea. The VA often denies such cases initially, but it doesn’t mean you should give up!
Learn how to make a disability claim and navigate the VA system with our free book, written by a VA attorney with decades of experience in filing and winning disability claims. Download the free guide to the VA claims process!
Secondary Service Connection
When your sleep apnea is secondary to another service-connected condition, you will need to provide a medical nexus to link the two conditions, stating that your sleep apnea is “at least as likely as not” caused or aggravated by a service-connected condition, such as:
- Rhinitis, Sinusitis or Deviated Septum (chronic nasal obstruction)
- PTSD (causes disrupted breathing and may lead to weight gain due to medications)
- GERD (nighttime reflux affects the airway)
- Asthma or Chronic Bronchitis (breathing impairment)
- TBI (can affect the brain’s ability to control breathing, leading to Central Sleep Apnea)
The surge in obstructive sleep apnea diagnoses since the wars in Iraq and Afghanistan is due not only to physical injuries like TBI but also mental health sequelae such as PTSD, depression, and insomnia. The presence of these conditions has been shown to dramatically increase the risk of developing sleep apnea.
Veterans who have both OSA and PTSD often deal with insomnia, have a harder time sticking to CPAP treatment, and don’t respond as well to therapy. When insomnia is also present, it can make sleep apnea symptoms and overall health even worse. Many veterans don’t just have sleep apnea – they have several conditions, compounding the severity of their symptoms and the complexity of their claims.
Sleep Apnea from Toxic Exposure
Many veterans who served in Iraq, Afghanistan, and other deployment zones were exposed to particulate matter such as airborne toxins from burn pits, jet fuel, and industrial waste. While sleep apnea is not currently recognized as a presumptive condition, scientific evidence suggesting that toxic exposure causes chronic inflammation and damage to the airway can be used to win obstructive sleep apnea claims.
If veterans demonstrate that the sleep apnea was caused or aggravated by their time in service, they will be able to get it service-connected for benefits. This will require:
- Providing evidence of exposure (e.g., deployment location)
- Presenting a medical nexus letter linking their apnea to toxic exposure
- Submitting a formal diagnosis through a sleep study
Veterans are encouraged to include comorbid conditions, such as sinusitis, rhinitis, asthma, or bronchitis, which may have presumptive status and support a broader claim.
Case Example: Sleep Apnea Secondary to Sinusitis
Citation Nr. 1811519 (Feb. 23, 2018)
In this case on appeal from the VA Regional Office in Winston-Salem, North Carolina, Hill & Ponton successfully represented a veteran who served from April 1987 to September 1997 and later developed obstructive sleep apnea. The veteran argued that his sleep apnea was related to a nasal fracture in service or, alternatively, was secondary to his service-connected sinusitis. VA had diagnosed OSA years after service, and the record included conflicting medical opinions about whether chronic sinus issues can contribute to sleep apnea. Hill & Ponton focused the appeal on the secondary service connection theory and made sure the Board had a medically sound explanation that connected sinusitis to airway obstruction and worsening sleep apnea.
What Helped Win This Sleep Apnea Claim?
- Choosing the Best Legal Strategy. The veteran raised a nasal fracture theory, but there was a built-in problem: although he was service connected for an injury residual scar on the nose, service connection was not established for a nasal fracture. Hill & Ponton leaned into the better-supported pathway. The veteran already had service connection for sinusitis, and the remaining question was medical: did sinusitis cause or aggravate obstructive sleep apnea?
- Using a Strong Medical Rationale. In April 2016 an examiner opined the sleep apnea was less likely related to a nasal fracture. Then in June 2016, the same examiner stated it was at least as likely as not that the veteran’s sleep apnea was aggravated beyond its natural progression by his service-connected sinusitis. He explained that chronic sinusitis can obstruct nasal passages, reducing airflow in and out of the lungs, which aggravates breathing problems and contributes to worsened sleep apnea. This was the key link for secondary service connection.
- Undercutting a Weak VA Opinion. In September 2017, another examiner stated that sleep apnea was diagnosed several years after service and that there was no clinical correlation between OSA and a chronic nasal issue. But the Board determined that focusing on the time gap is more relevant to direct service connection than secondary service connection, and that the opinion’s “no correlation” statement did not address the rationale provided in June 2016.
Did VA Deny Your Disability Claim?
Let our team review your case today!
START your free evaluation todayHow to File a VA Disability Claim for Sleep Apnea
Filing a VA disability claim involves gathering extensive medical and lay evidence, understanding how your condition is rated, and submitting the appropriate forms.
- File VA Form 21-526EZ. This begins your claim and should list “sleep apnea” as the condition. If it is secondary to another condition (like PTSD), be sure to indicate that. The form can be filed online on va.gov, at a VA regional office or with the help of a Veterans Service Organization (VSO).
- Provide a Formal Diagnosis. VA requires a sleep study for rating purposes (without it, your sleep apnea claim will almost certainly be denied). This can be from a VA facility or a private provider, but it must include objective findings (e.g., AHI score, CPAP prescription).
- Build Your Nexus. If you’re claiming direct service connection, submit service treatment records or lay statements showing in-service symptoms. If claiming secondary service connection, a medical opinion (nexus letter) from a provider linking the sleep apnea to another service-connected condition is essential.
- Submit Supporting Evidence. Provide treatment records of any sleep problems and CPAP use, buddy statements that corroborate snoring or breathing events during sleep in service, lay statements from family and any other evidence that can show symptoms manifested or worsened during active duty service.
- Attend the C&P Exam. The Compensation & Pension exam is where the VA may evaluate your current condition. Be honest, detailed, and clear about your symptoms and how they impact your life.
What Happens During the C&P Exam for Sleep Apnea?
- Review of medical records and sleep study history
- Interview about symptoms, onset, and course
- Treatment review (CPAP, oral appliance, surgery)
- Risk factors review (weight history, smoking, alcohol, anatomy, nasal obstruction)
- Short physical exam (often includes ENT/airway observations and vitals)
Most VA sleep apnea exams are completed using the Sleep Apnea Disability Benefits Questionnaire. The examiner may be a physician, nurse practitioner, or physician assistant. This medical evaluation is meant to determine two things:
- Do you currently have sleep apnea, and how is it treated?
- Is the sleep apnea at least as likely as not related to service or to another service-connected condition
What Is the Examiner Looking for?
1. Diagnosis and Objective Testing
You will need a sleep study in the record (in-lab polysomnogram or home sleep apnea test), otherwise the examiner will generally not be able to confirm obstructive sleep apnea as a diagnosis for rating purposes. The examiner will usually confirm:
- The date and type of sleep study
- Results, often including the AHI (apnea-hypopnea index) and oxygen desaturation findings
- Whether the diagnosis is OSA vs central sleep apnea or mixed
2. Symptoms
- Loud snoring, witnessed apneas, choking/gasping
- Non-restorative sleep, morning headaches
- Daytime sleepiness, fatigue, concentration issues
- Driving/work safety issues
3. Complications (if they exist)
- Hypertension, heart disease, stroke history
- Weight/BMI and neck circumference (often relevant to OSA risk)
- Nasal obstruction, deviated septum, chronic rhinitis/sinusitis
- Mental health symptoms that affect sleep (insomnia is common but distinct)
4. Treatment (especially CPAP use)
VA ratings for sleep apnea heavily track whether treatment requires a breathing device. Bring your CPAP compliance report, if you have it, and expect questions on:
- CPAP/BiPAP prescription date
- Mask type and settings (if known)
- Adherence and tolerance (hours/night, problems, side effects)
- Whether symptoms improve with CPAP
- If CPAP is prescribed but not tolerated, what alternatives are used (oral appliance, surgery, positional therapy)
Getting a Better VA Rating
The most common ratings for sleep apnea in veterans is 30%, or 50% if a CPAP is required. But you can increase your total rating by appealing the VA decision or by filing new claims for related conditions that contribute to sleep apnea or make it worse. You could get a higher rating for:
- Severe respiratory symptoms or declining lung function
- CPAP intolerance with worsening symptoms
- Secondary conditions
- TDIU (Total Disability based on Individual Unemployability)
Unhappy with your VA rating? Contact us for a free review
Winning Case Example: Rating for CPAP Use
In this case, a veteran sought an increased disability rating for his respiratory issues. The veteran was using a CPAP machine to treat his obstructive sleep apnea and did receive a 50% disability rating from the date the CPAP machine was prescribed (January 2010), but argued that his condition warranted a higher disability rating. The Board of Veterans’ Appeals reviewed the evidence and ultimately awarded a 60% disability rating for sarcoidosis (up from the previously assigned 50% rating for CPAP use), starting with the date of February 16, 2016.
How the Veteran Qualified for a 60% Rating
- The veteran’s February 2016 pulmonary function test results were significant in securing a higher rating. His DLCO (a measure of lung function) dropped to 55%, which meets the criteria for a 60% disability rating under Diagnostic Code 6600 (sarcoidosis).
- The Board noted the veteran’s credible lay statements, including testimony from a Board hearing, where he described his dependency on the CPAP machine and the challenges he faced without it. These statements, alongside his medical records, solidified the claim.
This case highlights the importance of providing both medical and lay evidence when seeking a higher disability rating for sleep apnea requiring a CPAP machine. While a CPAP machine alone may warrant a 50% rating, more severe symptoms, such as declining lung function, can lead to a higher rating. In this case, the veteran successfully secured a 60% rating by demonstrating a worsening of his condition.
Sleep apnea affects countless veterans and is often overlooked, misdiagnosed, or wrongly rated. Whether your condition is due to trauma, mental health, or toxic exposure, you deserve to be recognized and compensated. Hill & Ponton believes in arming disabled veterans with the knowledge and the tools to succeed. We offer free resources and evaluations of previously denied or underrated claims, with no strings attached. Get a free case evaluation from us today!
Conditions Linked to Sleep Apnea
- PTSD – Can disrupt sleep patterns, increase arousal, and lead to insomnia, all of which may worsen or trigger sleep apnea. Medications used for PTSD may also interfere with breathing regulation.
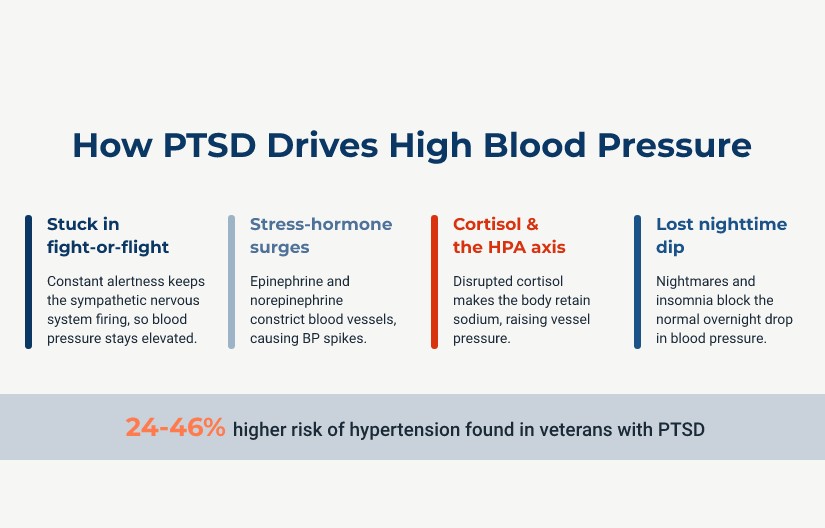
- Hypertension – Often secondary to sleep apnea, as repeated oxygen drops during apneic events can raise blood pressure. Untreated sleep apnea is a known contributor to chronic hypertension.
- Depression and Anxiety Disorders – These conditions often disrupt sleep and increase insomnia, which can worsen sleep apnea symptoms or reduce treatment effectiveness.
- Chronic Pain – Pain can interfere with sleep, and medications (especially opioids) used to treat pain may depress breathing, increasing the risk of sleep apnea.
- Diabetes Mellitus – Sleep apnea increases insulin resistance and is a known risk factor for developing type 2 diabetes.
- Asthma and other respiratory conditions – Chronic airway inflammation and reduced lung function can make breathing during sleep more difficult, increasing apnea risk.
- Traumatic Brain Injury – TBI can damage the brain’s ability to regulate breathing, leading to central sleep apnea or worsening existing sleep-disordered breathing.
- Gastroesophageal Reflux Disease (GERD) – Acid reflux can irritate the airway and worsen nighttime breathing problems, while apnea can also exacerbate reflux symptoms.
- Obesity – Extra tissue around the neck and upper airway can physically block airflow during sleep, making obesity the most common risk factor for obstructive sleep apnea. While obesity is not recognized as a disability per se, when it is caused by a service-connected condition (such as back pain) it can be used as an intermediate step to establish service connection for other disabilities, including sleep apnea.
- Neck or Upper Airway Injuries – Trauma or injury to these areas can narrow or obstruct the airway, leading to or worsening obstructive sleep apnea.
- Sinusitis or Rhinitis – Chronic nasal congestion and inflammation can reduce airflow and lead to mouth breathing, increasing apneic events.
- Chronic Fatigue Syndrome – Sleep apnea can worsen fatigue and non-restorative sleep, overlapping significantly with chronic fatigue symptoms.
- Migraines and Headaches – Poor sleep quality and oxygen deprivation from apnea can trigger or worsen morning headaches and migraines.
- Heart Conditions – Apneic episodes stress the cardiovascular system, contributing to arrhythmias, heart failure, and other cardiac complications
Maximizing your VA rating should involve a personalized and strategic approach to connecting secondary conditions to your primary diagnosis based on your personal medical history. Make sure you provide sleep studies, doctor’s notes and records of treatments for sleep apnea and any linked conditions, as well as detailed personal records of how your sleep apnea and secondary conditions affect your daily life, focusing on their interconnectedness.
Learn to Prepare (and Win!) Your VA Claim with Our Free Book
The Road to VA Compensation Benefits
Sleep apnea affects countless veterans and is often overlooked, misdiagnosed, or wrongly rated. Whether your condition is due to trauma, mental health, or toxic exposure, you deserve to be recognized and compensated. Hill & Ponton believes in arming disabled veterans with the knowledge and the tools to succeed. We offer free resources and evaluations of previously denied or underrated claims, with no strings attached. Get a free case evaluation and we’ll point you in the right direction!
TDIU: the Path to 100% VA Disability for Sleep Apnea
TDIU stands for Total Disability Based on Individual Unemployability (TDIU) and it provides 100% disability compensation to veterans with a lower rating who, due to their disability, cannot earn enough to make a living. To qualify for TDIU you must a) have one service-connected disability rated at 60% or more, OR b) have two or more disabilities with one rated at 40% or more and a combined rating of at least 70%.
Additionally, disabled veterans who don’t meet either of these thresholds can still qualify for TDIU under 38 C.F.R. § 4.16(b) if they cannot maintain substantially gainful employment (defined by the VA as earning more than the poverty threshold and not considered sheltered or marginal).
How Hill & Ponton Won TDIU for a Veteran with Sleep Apnea
Citation Nr: 1429555 (June 30, 2014)
In this case on appeal from Jackson, Mississippi, Hill & Ponton represented a veteran who served from April 1978 to December 1992. Years after service, the veteran was diagnosed with obstructive sleep apnea and argued it was related to his already service-connected nasal trauma that left him with a nasal pyramid and septal deformity and partial obstruction. He also sought TDIU because his service-connected mental health and physical conditions had made steady work impossible. The VA initially denied the veteran.
The VA record included conflicting medical opinions about whether a deviated septum can cause sleep apnea. Hill & Ponton focused on a sleep apnea diagnosis confirmed by testing, a documented service-connected nasal obstruction, and a strong medical opinion that directly addressed causation and risk factors. At the same time, the firm developed evidence showing the veteran’s service-connected conditions prevented substantially gainful employment, especially given medication side effects and mental health limitations.
What Helped Win These Claims?
Strong Nexus Linking Sleep Apnea to Service-Connected Nasal Trauma
The veteran was diagnosed with obstructive sleep apnea after a June 2009 sleep study that followed a history of loud snoring, witnessed apneas, daytime sleepiness, and non-restorative sleep. The appeal then turned on whether his service-connected nasal trauma and resulting airway obstruction could be medically tied to his sleep apnea.
Two VA examinations in March 2012 disagreed in part. One examiner opined it was 50 percent likely that the veteran’s mild sleep apnea was secondary to nasal trauma that caused nasal airway obstruction. Another examiner disagreed that a deviated septum is causative, but still acknowledged a deviated septum is an aggravating factor for obstructive sleep apnea.
Hill & Ponton strengthened the record with a November 2013 opinion from a private pulmonologist who reviewed the file and concluded it was at least as likely as not that the veteran’s obstructive sleep apnea was caused by the service-connected nasal trauma. The pulmonologist cited medical literature identifying deviated septum as a risk factor for sleep apnea and also noted the record showed other risk factors but did not show obesity. The Board found this positive specialist opinion persuasive and granted service connection for sleep apnea as secondary to nasal trauma.
Proving Unemployability with a Vocational Expert Opinion and Work History
For TDIU, the veteran already had significant service-connected disabilities in addition to sleep apnea, including dysthymic disorder rated 70 percent, a cervical spine disability rated 20 percent, nasal trauma rated 10 percent, right carpal tunnel syndrome rated 10 percent, and bilateral tinnitus rated 10 percent. His combined rating was 80 percent, meeting the schedular threshold for TDIU consideration.
The veteran had last worked as a security officer in July 2006. He attempted to work as a flea market vendor in 2006 and 2007 but had to stop because of his medical conditions. Hill & Ponton used this work history to show that the veteran could not maintain consistent employment even in less demanding roles.
A private vocational expert reviewed the record in December 2013 and opined that it was at least as likely as not, to a high degree of vocational certainty, that the veteran’s service-connected dysthymic disorder and cervical spine disorder prevented him from performing any substantially gainful work. The opinion also emphasized that medication for neck pain precluded driving for 12 hours and that the combined side effects of psychiatric and pain medication could periodically prevent activities requiring mental alertness, clear judgment, and physical coordination.
See how We Helped other veteransSleep Apnea Ratings FAQ
Yes, especially if you can show symptoms during service or link the condition secondarily to another service-connected disability.
Yes. A diagnosis from a sleep study is generally required for VA to confirm the presence of sleep apnea and consider the condition for compensation.
Yes, if you have persistent daytime hypersomnolence, you may still qualify for 30%. But without treatment or CPAP, it’s harder to get higher ratings unless other complications are present.
Under current rules, yes. However, proposed VA changes would eliminate this automatic 50% rating and require documented functional impairments. Veterans should prepare for this potential change and secure their rating as soon as possible. Stay updated on VA news.
Download CPAP usage data or ask your provider to print usage logs that will show compliance, which helps validate your 50% rating and future care needs.
The VA could reduce your rating if you stop using prescribed treatment without medical justification. Always document reasons (e.g., side effects or doctor-advised discontinuation).
No. The proposed changes will not affect veterans who already have a service-connected sleep apnea rating or those who file a claim before the changes go into effect. It can however affect those who later reopen the claim.
If you have new and material evidence, such as a sleep study or medical opinion, you can file a Supplemental Claim to reopen the case.
Did VA Deny Your Disability Claim?
Let our team review your case today!
START your free evaluation todayWritten by